

- Gamer’s syndrome aslo known as De Quervain’s Tenosynovitis is a painful inflammation of tendons on the side of the wrist at the base of the thumb.
- These tendons include the extensor pollicis brevis (EPB) and the abductor pollicis longus (APL). These muscles are located on the dorsal side of the forearm and go to the lateral side of the thumb through a fibrous-osseous tunnel made of the processus styloideus radii and the extensor retinaculum.
 |
| de Quervain's Tenosynovitis |
Anatomy related to Gamer’s syndrome
- The tendon sheaths around the abductor pollicis longus and extensor pollicis brevis pass through the fibro-osseous tunnel located along the radial styloid at the distal wrist.
M. extensor pollicis brevis (EPB)
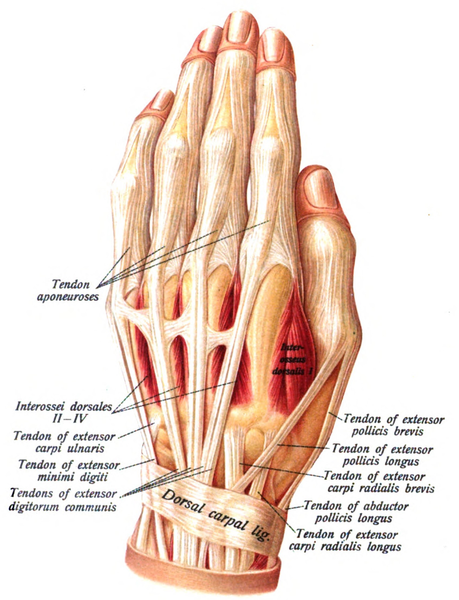
- Origin: ½ dorsal side of the radius, the interossea membrane
- Insertion: base of the proximal phalanx of the thumb
- Function: wrist joint radial abduction and thumb extension
- Innervations: Radial nerve
- Artery: A. interossea posterior
M. abductor pollicis longus (APL)
- Origin: dorsal side of the radius and the ulna, the membrana interossea
- Insertion: base of ossis metacarpi I
- Function:wrist joint: radial abduction, thumb abduction
- Innervations: radial nerve
- Artery: A. interossea posterior
Causes of Gamer’s syndrome
- De Quervain’s Tenosynovitis as been attributed to myxoid degeneration (the process in which the connective tissues are replaced by a gelatinous substance) with fibrous tissue deposits and increased vascularity rather than acute inflammation of the synovial lining.
- This deposition results in thickening of the tendon sheath, painfully entrapping the abductor pollicis longus and extensor pollicis brevis tendons.
- It is associated with repetitive wrist motion, specifically motion requiring thumb radial abduction and simultaneous extension and radial wrist deviation.
- The classic patient population is mothers of newborns who are repeatedly lifting a newborn with thumbs radially abducted and wrists going from ulnar to radial deviation.
- The most common cause is chronic overuse.
- Activities such as golfing, playing the piano, fly fishing, carpentry, office workers and musicians can lead to chronic overuse injuries.
- Repetitive gripping, grasping, clenching, pinching, or wringing of objects can cause inflammation of the tendons and tendon sheaths and narrows the first dorsal compartment and causes limitation of motion of the tendons.
- If left untreated, the inflammation and progressive narrowing (stenosis) can lead to scarring that further limits thumb motion.
Symptoms of Gamer’s syndrome
- The primary complaint is radial sided wrist pain that radiates up the forearm with grasping or extension of the thumb.
- The pain has been described as a “constant aching, burning, pulling sensation.” Pain is often aggravated by repetitive lifting, gripping, or twisting motions of the hand.
- Swelling in the anatomical snuff box, tenderness at the radial styloid process, decreased CMC abduction ROM of the 1st digit, palpable thickening of the extensor sheaths of the 1st dorsal compartment and crepitus of the tendons moving from the extensor sheath may be found upon examination.
- Other possible findings include weakness and paresthesia in the hand.
- Finkelstein’s diagnostic test will present positive provoking the patient’s symptoms.
Diagnosis of Gamer’s syndrome
HISTORY
- Overuse injury vs acute trauma
- Prior history of symptoms
- Repetitive movements of the upper extremity with work or activities of daily living (ADL)
- Pain localized over the base of the thumb and dorsolateral aspect of the wrist near radial styloid process
- Hand dominance
- Pregnant or currently in the post-partum stage
EXAMINATION
- Patients present with radial-sided wrist pain which is typically worsened by thumb and wrist motion.
- The condition may be associated with pain or difficulty with tasks such as opening a jar lid.
- Tenderness overlying the radial styloid is usually present, and fusiform swelling in this region may also be appreciated.
- On palpation some key, significant findings will be tenderness over the base of the thumb and/or 1st dorsal compartment extensor tendons on the thumb side of wrist particularly over the radial styloid process
Finkelstein’s test
- To begin, the patient must sit comfortable and relaxed on the examination table. Next, examine the patients hand in the air, while the other hand rests just beside the body. The therapist then asks the patient to make a fist around a thumb and to perform a ulnar deviation.
- A modified version of the test is that the patient must sit comfortable and relaxed on the examination table. The patient must hold his afflicted hand in the air, while the other hand should be resting against his/ her body.
- The therapist grasps the afflicted hand of the patient and rotates it in ulnar deviation. He pulls the patient’s thumb across the palm of his/ her hand. This causes additional stress on the extensor tendons of the thumb.
- The patient actively (or active assistive) flexes thumb maximally and wraps fingers over thumb, making a fist. The patient then ulnarly deviates his/her wrist to stretch the muscles of the 1st extensor compartment. The test is positive if the patient complains of pain over the 1st extensor compartment of the wrist.
- Interpretation
- Negative result: The patient doesn’t feel any pain radiating up the inside of his/ her arm from the thumb.
- Positive result: Ask the patient if he or she feels pain radiating up the inside of his or her arm from the thumb. If the patient reports noticeable pain then, the Finkelstein’s test is positive, what indicates De Quervain’s syndrome
Medical management of Gamer’s syndrome
- De Quervain tendinopathy can be self-limited and may resolve without intervention.
- For those individuals with persistent symptoms, splinting, systemic anti-inflammatories and corticosteroid injection are the most frequently utilized non-surgical treatment options.
- Splinting with a thumb spica brace may offer patients temporary relief, but failure and recurrence are often high and compliance lo
- Non-Surgical Treatment
- The aim of non-surgical management is to reduce pain and swelling; initial treatment of de Quervain’s tenosynovitis may include:
- Immobilizing your thumb and wrist with a splint or brace to help rest your tendons. Clinicians do not agree on the frequency and duration of the splint; some think it should be worn continually for four to six weeks; others recommend wearing it only as needed for pain.
- Avoiding repetitive or aggravating movements
- Applying ice to the affected area
- Nonsteroidal anti-inflammatory drugs (NSAID)
- Patients may also be prescribed
- for immobilization up to 6 weeks. A splint for thumb immobilization can do this. When used a improvement was observed but when they combined it with NSAID’s they found an even bigger improvement of .
- Ultrasound is though to improve the treatment outcome and can be used as a diagnostic tool in the management of de Quervain’s disease .Success with ultrasound-guided injections was better than it was reported in the literature and without adverse reactions.
- Ultrasound-guided injections targeting the M. Extensor Pollicis Brevis with septation is more effective than manual injection.
Surgical treatment of Gamer’s syndrome
- Surgery is rare and is usually for those when non-surgical treatment has failed and the patient experiences persistent inflammation affecting his or her function. The goal of surgery is to open the dorsal compartment covering to make more room for the irritated tendons. The opening allows pressure relief of the tendons, to ultimately restore free tendon gliding.
- Corticosteroid injection has been reported to provide near-complete relief with one or two injections. The injection is performed into the tendon sheath about 1 cm proximal to the radial styloid where the tendons are palpable.
- If symptoms fail to improve or recur after two corticosteroid injections, operative management is an option. Surgery is usually performed in an outpatient setting. It can entail local, regional or general anaesthesia.
- Post-operative care is usually limited. A simple dressing or wrap is frequently utilized with no need for complex wound care. Patients are advised to begin early use for activities of daily living and other light activities. Once sutures are removed, usually by two weeks, patients are typically released to resume normal activities. Patients may continue to experience mild swelling and tenderness at the surgical site for a few months.
Physiotherapy management of Gamer’s syndrome
- ICE PACK / HOT PACK – Heat can help relax and loosen tight musculature, and ice can be used to help relieve inflammation of the extensor sheath.
- ULTRASOUND THERAPY :Ultra Sound is therapeutic modalities which generate ultra sound causes deep heat, which provides micro massage to soft tissue,increase flexibility ,promotes healing of tissue as well improve localised blood supply to area.and ultimately pain relief.
- MASSAGE – Deep tissue massage at the thenar eminence can help relax tight musculature that causes pain. Graston Technique of manual soft tissue mobilization along with the eccentric exercise is also helpful.
- Graston technique includes breaking down fascia restriction, stretching connective tissue and promoting better healing environment.
- STERTCHING – Stretching the thenar eminence muscles into thumb extension and abduction can relax and lengthen this tight musculature that causes pain.
Increasing Strength
- Resisted finger and thumb extension
- Palm up position – for thumb extension and abduction strength
- Thumb up position – for thumb extension and abduction strength
- Resisted radial deviation
- In thumb up position
- Resisted supination
- In thumb up position
- Resisted thumb opposition
- In thumb up position
- Improving Range of Motion Stretching as explained above can be used to improve range of motion. Ice/Heat packs can relax tight musculature so that you can attain a bigger range of motion.
- Mobilization with movement has shown effectiveness in decreasing the pain, improving range of motion and improving the function of a patient with De-Quervain tenosynovitis. The therapist provides a manual radial glide of the proximal row of carpals, then asked the patient to move her thumb into radial abduction-adduction.
- Mobilization with movement performed for 3 sets of 10 repetitions and followed by eccentric hammer curl exercise with theraband and high voltage electrical stimulation has shown effective result after 6 months followup.

- Kinesio-taping Technique can also be used to decrease pain and improve function.

0Comments