


This guide provides a structured approach to chest X-ray interpretation and includes examples of relevant pathology.
 |
| Chest X-ray Interpretation |
Confirm details
Begin chest X-ray interpretation by checking the following details:
- Patient details: name, date of birth and unique identification number.
- Date and time the film was taken
- Previous imaging: useful for comparison.
Assess image quality
Next, you should assess the quality of the image: a mnemonic you may find useful is ‘RIPE’.
Rotation
The medial aspect of each clavicle should be equidistant from the spinous processes.
The spinous processes should also be in vertically orientated against the vertebral bodies.
Inspiration
The 5-6 anterior ribs, lung apices, both costophrenic angles and the lateral rib edges should be visible.
Projection
Note if the film is AP or PA: if there is no label, then assume it’s a PA film (if the scapulae are not projected within the chest, it’s PA).
Exposure
The left hemidiaphragm should be visible to the spine and the vertebrae should be visible behind the heart.
ABCDE approach
The ABCDE approach can be used to carry out a structured interpretation of a chest X-ray:
- Airway: trachea, carina, bronchi and hilar structures.
- Breathing: lungs and pleura.
- Cardiac: heart size and borders.
- Diaphragm: including assessment of costophrenic angles.
- Everything else: mediastinal contours, bones, soft tissues, tubes, valves, pacemakers and review areas.
Video Guide to ABCDE approach
Part: 1
Part: 2
Watch Full Playlist:
Airway
Trachea
Inspect the trachea for evidence of deviation:
- The trachea is normally located centrally or deviating very slightly to the right.
- If the trachea appears significantly deviated, inspect for anything that could be pushing or pulling the trachea. Make sure to inspect for any paratracheal masses and/or lymphadenopathy.
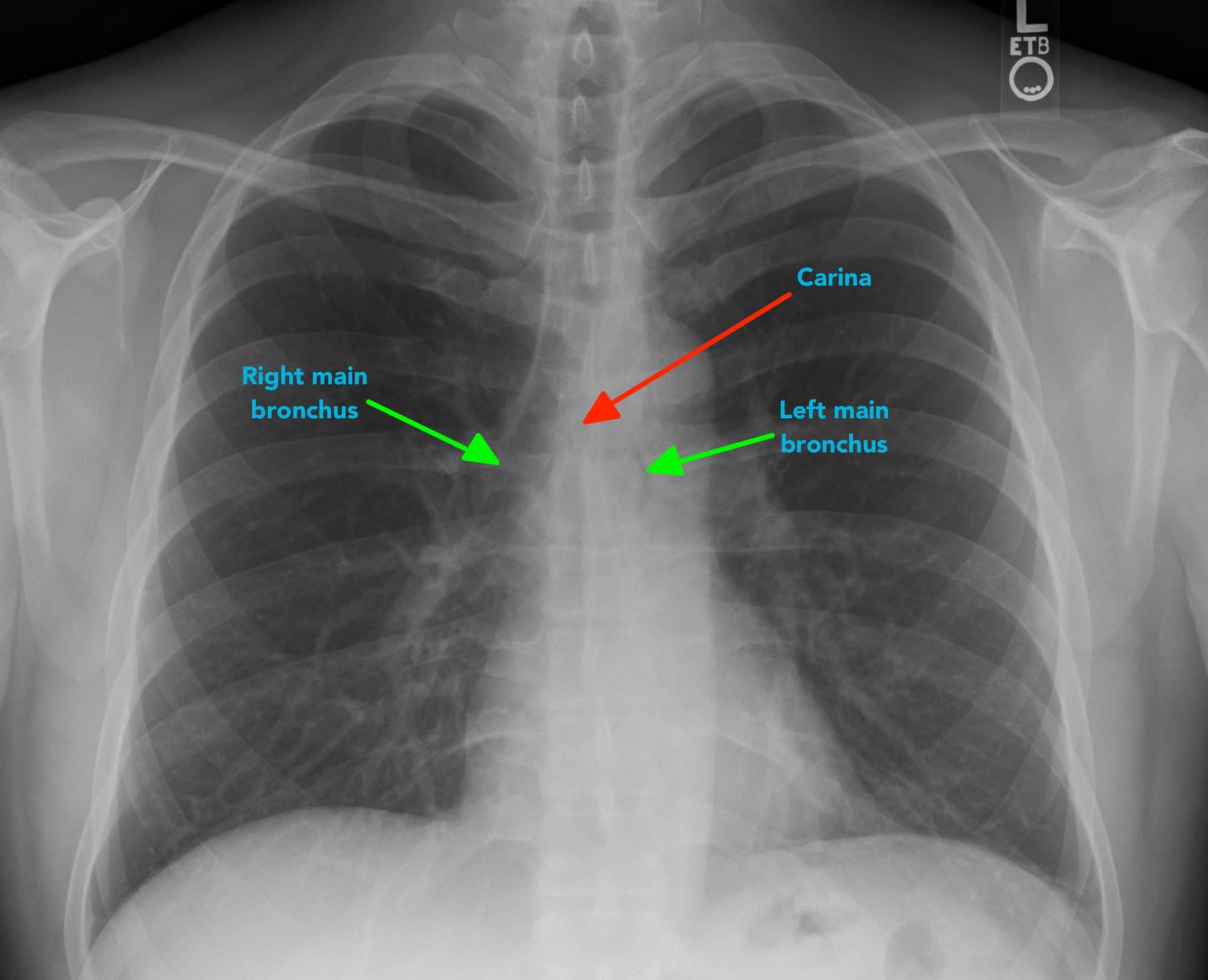
Carina and bronchi
The carina is cartilage situated at the point at which the trachea divides into the left and right main bronchus.
On appropriately exposed chest X-ray, this division should be clearly visible. The carina is an important landmark when assessing nasogastric (NG) tube placement, as the NG tube should bisect the carina if it is correctly placed in the gastrointestinal tract.
The right main bronchus is generally wider, shorter and more vertical than the left main bronchus. As a result of this difference in size and orientation, it is more common for inhaled foreign objects to become lodged in the right main bronchus.
Depending on the quality of the chest X-ray you may be able to see the main bronchi branching into further subdivisions of bronchi.
Hilar structures
The hilar consist of the main pulmonary vasculature and the major bronchi.
Each hilar also has a collection of lymph nodes which aren’t usually visible in healthy individuals.
The left hilum is often positioned slightly higher than the right, but there is a wide degree of variability between individuals.
The hilar are usually the same size, so asymmetry should raise suspicion of pathology.
The hilar point is also a very important landmark; anatomically it is where the descending pulmonary artery intersects the superior pulmonary vein. When this is lost, consider the possibility of a lesion here (e.g. lung tumour or enlarged lymph nodes).
Breathing
Lungs
Inspect the lungs for abnormalities:
- When interpreting a chest X-ray you should divide each of the lungs into three zones, each occupying one-third of the height of the lung.
- These zones do not equate to lung lobes (e.g. the left lung has three zones but only two lobes).
- Inspect the lung zones ensuring that lung markings are present throughout.
- Compare each zone between lungs, noting any asymmetry (some asymmetry is normal and caused by the presence of various anatomical structures e.g. the heart).
- Some lung pathology causes symmetrical changes in the lung fields, which can make it more difficult to recognise, so it’s important to keep this in mind (e.g. pulmonary oedema).
- Increased airspace shadowing in a given area of a lung field may indicate pathology (e.g. consolidation/malignant lesion).
- The complete absence of lung markings should raise suspicion of a pneumothorax.

Pleura
Inspect the pleura for abnormalities:
- The pleura are not usually visible in healthy individuals. If the pleura are visible it indicates the presence of pleural thickening which is typically associated with mesothelioma.
- Inspect the borders of each lung to ensure lung markings extend all the way to the edges of the lung fields (the absence of lung markings is suggestive of pneumothorax).
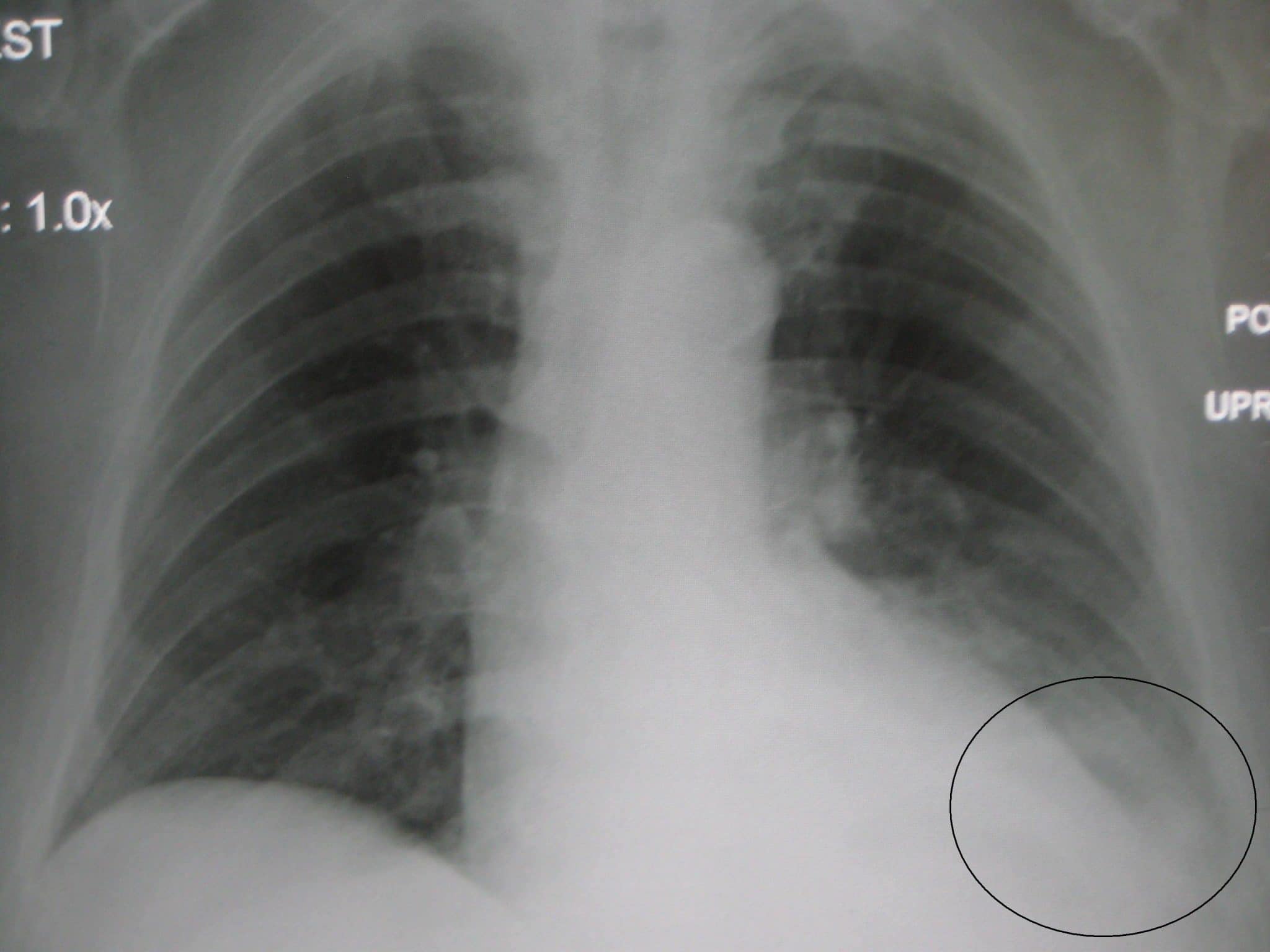
- Fluid (hydrothorax) or blood (haemothorax) can accumulate in the pleural space, resulting in an area of increased opacity on a chest X-ray. In some cases, a combination of air and fluid can accumulate in the pleural space (hydropneumothorax), resulting in a mixed pattern of both increased and decreased opacity within the pleural cavity.
Cardiac
Assess heart size
In a healthy individual, the heart should occupy no more than 50% of the thoracic width (e.g. a cardiothoracic ratio of less than 0.5).
This rule only applies to PA chest X-rays (as AP films exaggerate heart size), so you should not draw any conclusions about heart size from an AP film.
Cardiomegaly is said to be present if the heart occupies more than 50% of the thoracic width on a PA chest X-ray. Cardiomegaly can develop for a wide variety of reasons including valvular heart disease, cardiomyopathy, pulmonary hypertension and pericardial effusion.
Assess the heart’s borders
Inspect the borders of the heart which should be well defined in healthy individuals:
- The right atrium makes up most of the right heart border.
- The left ventricle makes up most of the left heart border.
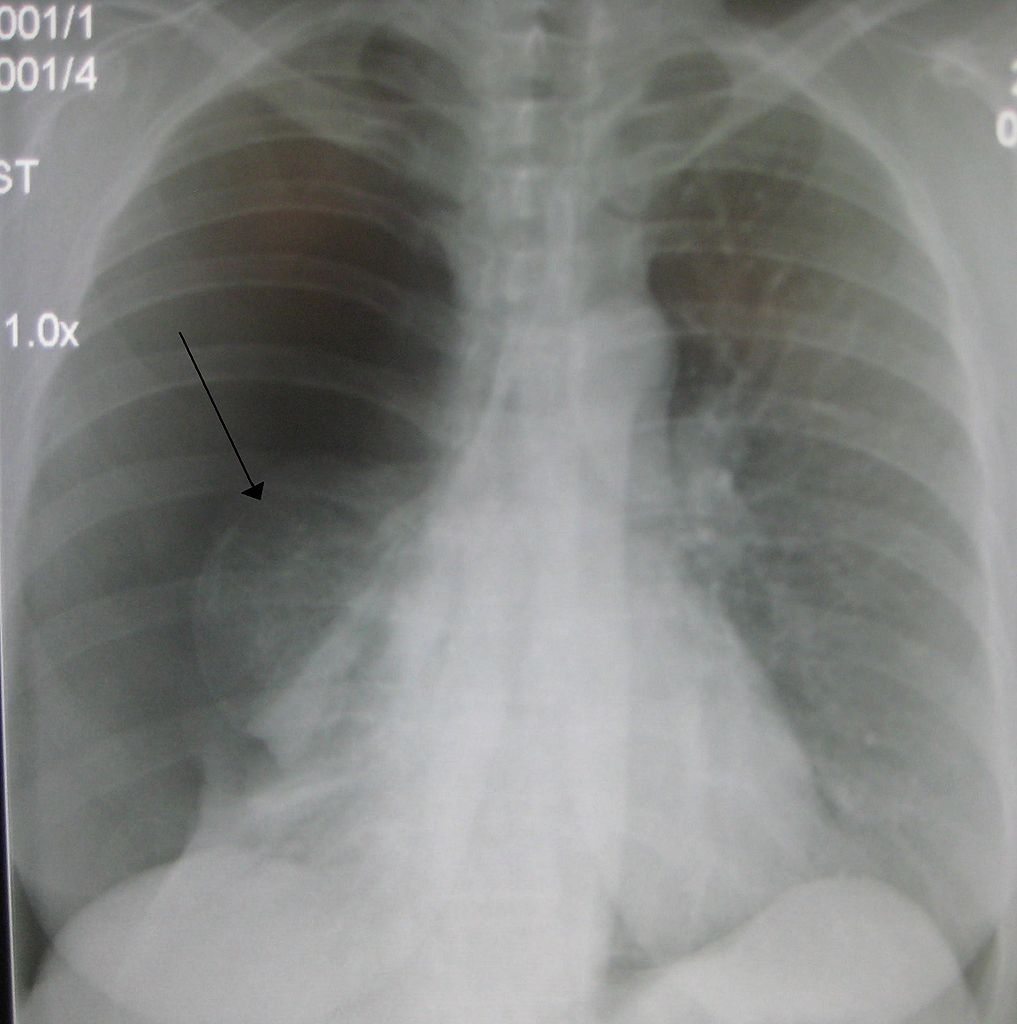
The heart borders may become difficult to distinguish from the lung fields as a result of pathology which increases the opacity of overlying lung tissue:
- Reduced definition of the right heart border is typically associated with right middle lobe consolidation.
- Reduced definition of the left heart border is typically associated with lingular consolidation.
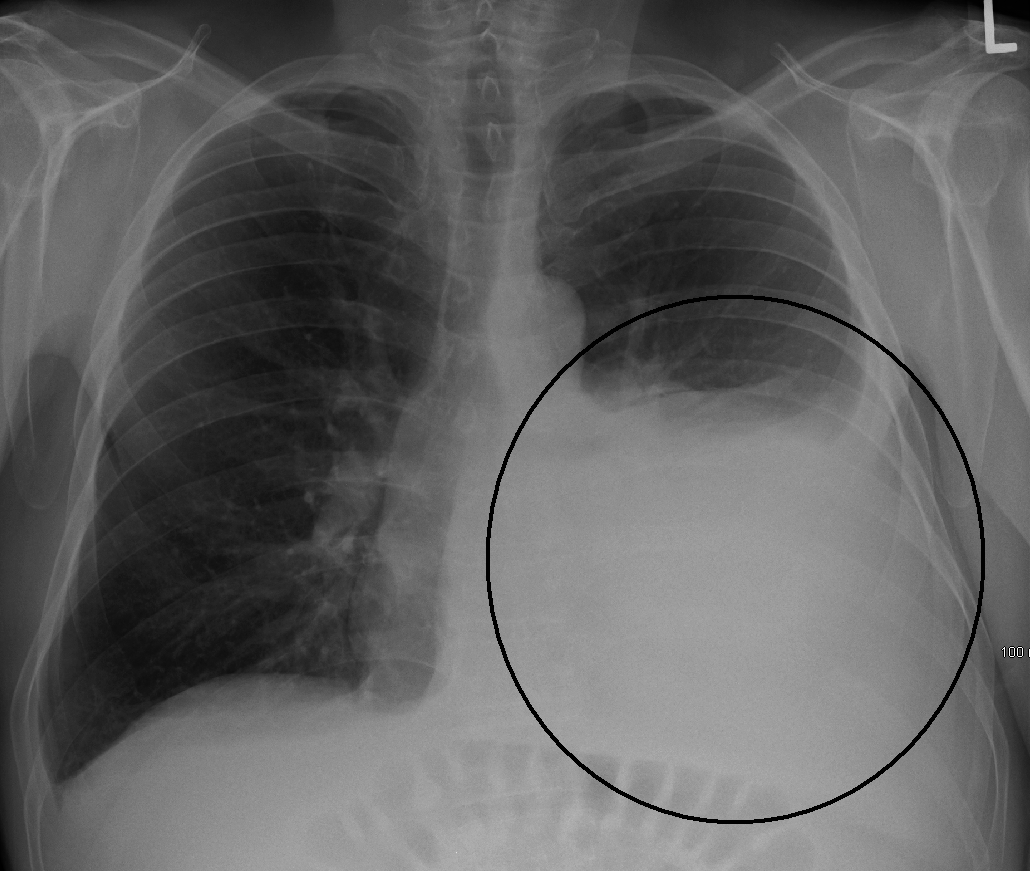
Diaphragm
The right hemidiaphragm is, in most cases, higher than the left in healthy individuals (due to the presence of the liver). The stomach underlies the left hemidiaphragm and is best identified by the gastric bubble located within it.
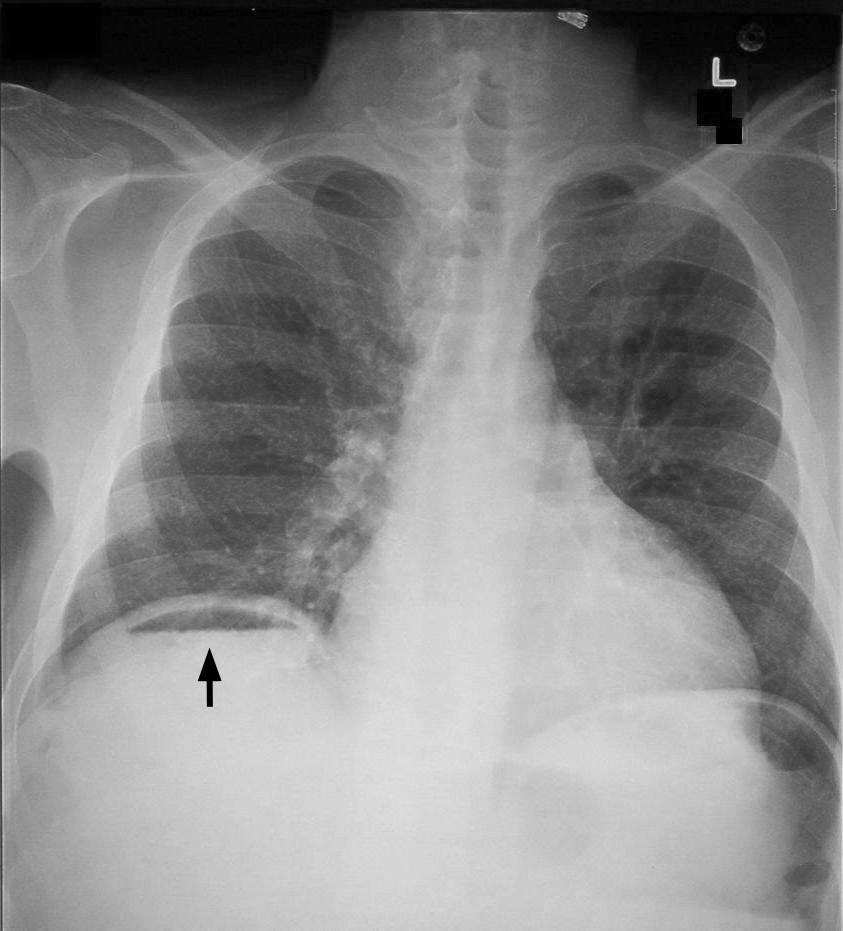
The diaphragm should be indistinguishable from the underlying liver in healthy individuals on an erect chest X-ray, however, if free gas is present (often as a result of bowel perforation), air accumulates under the diaphragm causing it to lift and become visibly separate from the liver. If you see free gas under the diaphragm you should seek urgent senior review, as further imaging (e.g. CT abdomen) will likely be required to identify the source of free gas.
There are some conditions which can result in the false impression of free gas under the diaphragm, known as pseudo-pneumoperitoneum, including Chilaiditi syndrome. Chilaiditi syndrome involves the abnormal position of the colon between the liver and the diaphragm resulting in the appearance of free gas under the diaphragm (because the bowel wall and diaphragm become indistinguishable due to their proximity). As a junior doctor, you should always discuss a scan that appears to show free gas with a senior colleague immediately.
Costophrenic angles
The costophrenic angles are formed from the dome of each hemidiaphragm and the lateral chest wall.
In a healthy individual, the costophrenic angles should be clearly visible on a normal chest X-ray as a well defined acute angle.
Loss of this acute angle, sometimes referred to as costophrenic blunting, can indicate the presence of fluid or consolidation in the area. Costophrenic blunting can also develop secondary to lung hyperinflation as a result of diaphragmatic flattening and subsequent loss of the acute angle (e.g. chronic obstructive pulmonary disease).
Everything else
Mediastinal contours
The mediastinum contains the heart, great vessels, lymphoid tissue and a number of potential spaces where pathology can develop. The exact boundaries of the mediastinum aren’t particularly visible on a chest X-ray, however, there are some important structures that you should assess.
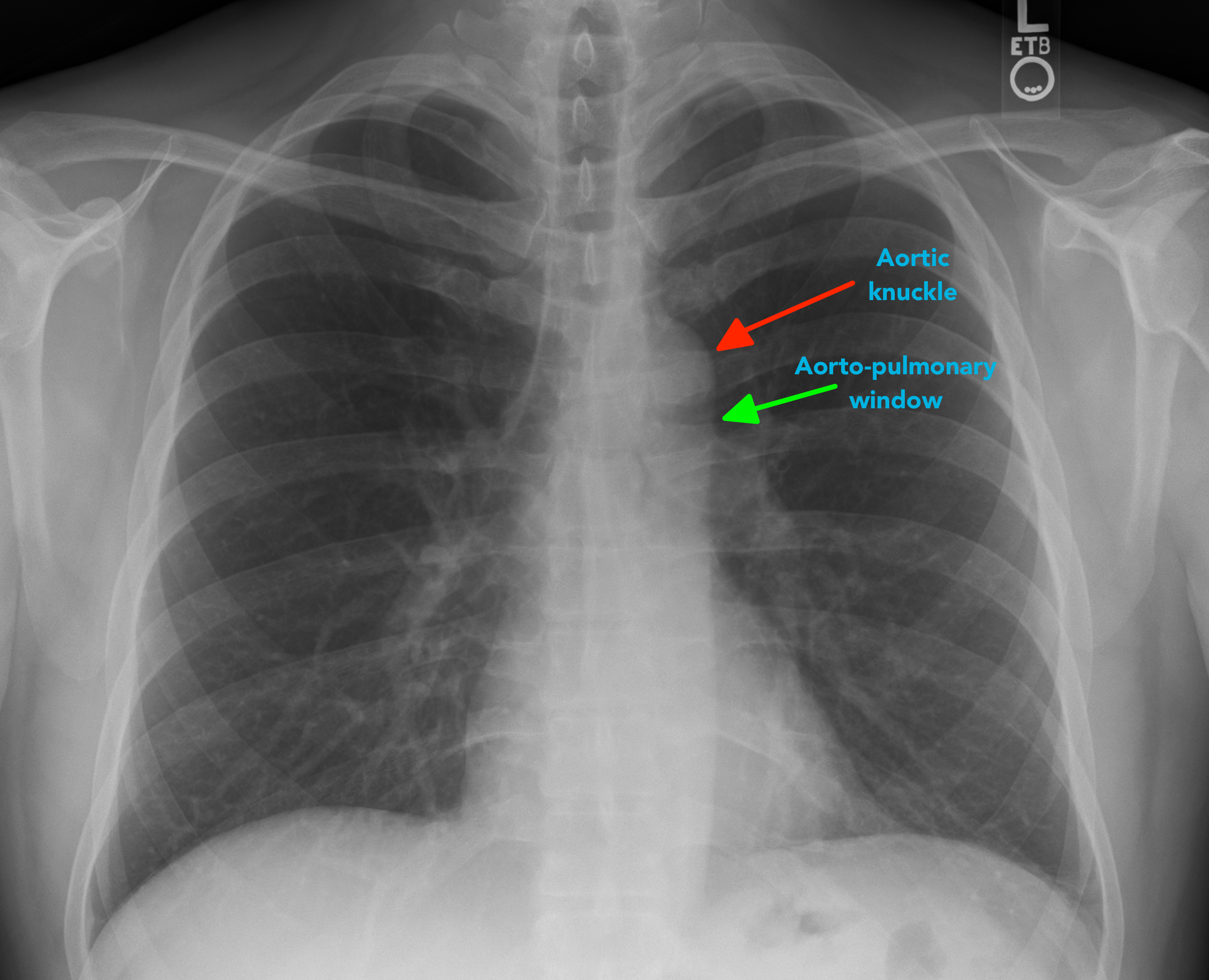
Aortic knuckle
The aortic knuckle is located at the left lateral edge of the aorta as it arches back over the left main bronchus. Reduced definition of the aortic knuckle contours can occur in the context of an aneurysm.
Aortopulmonary window
The aortopulmonary window is a space located between the arch of the aorta and the pulmonary arteries. This space can be lost as a result of mediastinal lymphadenopathy (e.g. malignancy).
Bones
Inspect the visible skeletal structures looking for abnormalities (e.g. fractures, lytic lesions).
Soft tissues
Inspect the soft tissues for obvious abnormalities (e.g. large haematoma).
Tubes, valves and pacemakers
Tubes
Nasogastric tube placement is something you’ll often be asked to assess on a chest X-ray to confirm safe placement for feeding. See our NG tube placement guide for more details.
Lines
Various tubes and cables will be visible as radio-opaque lines on the chest X-ray (e.g. central line, ECG cables).
Artificial heart valves
Artificial heart valves typically appear as ring-shaped structures on a chest X-ray within the region of the heart (e.g. aortic valve replacement).
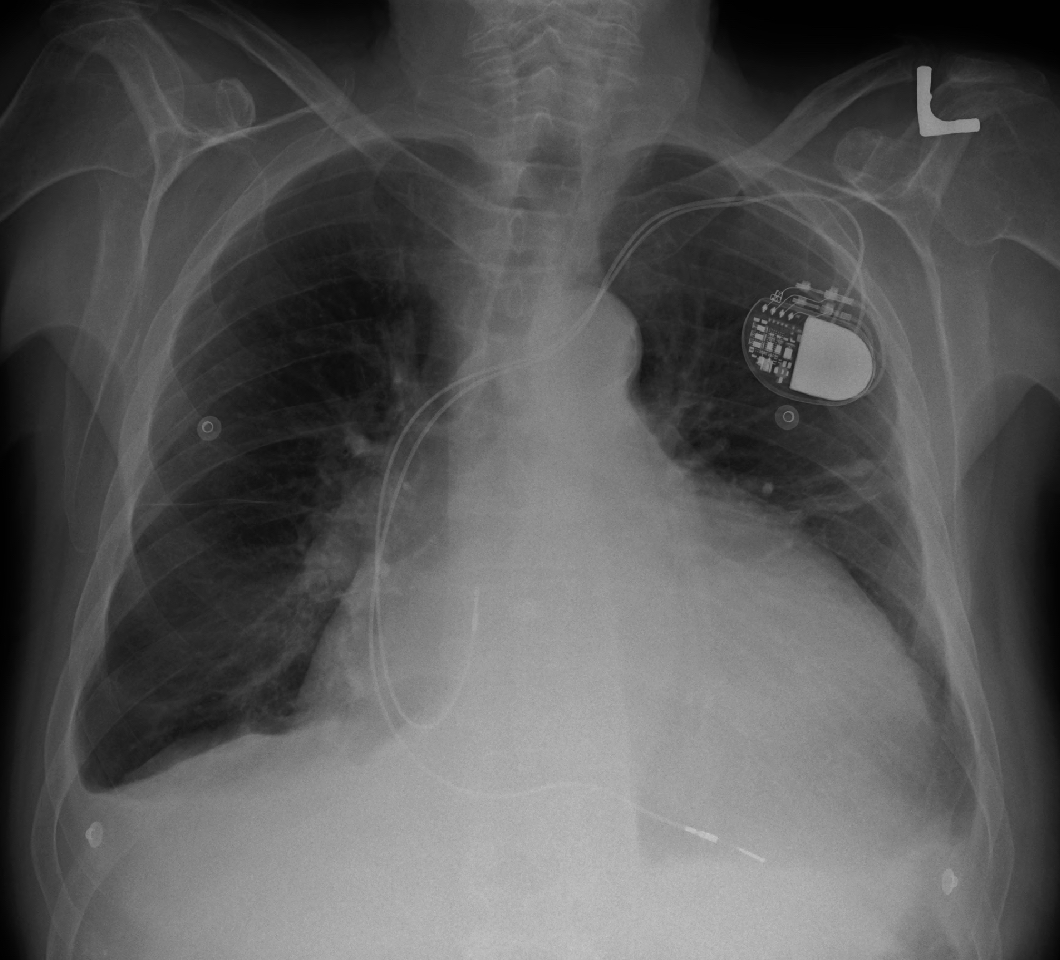
Pacemaker
Pacemakers typically appear as a radio-opaque disc or oval in the infraclavicular region connected to pacemaker wires which are positioned within the heart.
Review areas
Finally, before completing your assessment of a chest X-ray, make sure you’ve looked at the ‘review areas’ where pathology is often missed. These areas include:
- the lung apices
- the retrocardiac region
- behind the diaphragm
- the peripheral region of the lungs
- the hilar regions
This ensures you’ve comprehensively assessed the X-ray and reduces the risk of missing subtle pathology (e.g. a small nodule).
References
- James Heilman, MD. Right-sided pneumonia. Licence: CC BY-SA 3.0.
- James Heilman, MD. Cardiomegaly. Licence: CC BY-SA 3.0.
- Hellhoff. Pneumoperitoneum. Licence: CC BY-SA 3.0.
- Steven Fruitsmaak. Chilaiditi syndrome. Licence: CC BY-SA 3.0.
0 Comments